
Painless Contralateral Nerve Root Mobilisations - taking tension off
the system for nerve root pain

As many of you will remember, earlier we presented an article on the use of contralateral neurodynamic movements as a means of reducing tension in the nerve roots. This article takes the subject further by presenting exactly how to do this with lower limb movements in the case of neck pain. In this sequel, the physical mechanisms and various clinical techniques are discussed.
Rubenach (1985) found that 62% of asymptomatic subjects reported a reduction in the symptom response to the median neurodynamic test 1 (MNT1) with performance of a contralateral MNT1. If we consider that tension in the nervous system is key the mechanism of symptoms with the MNT1, adding more tension to the nervous system with a contralateral neurodynamic movement should theoretically increase symptoms with the contralateral test. But, since the symptoms often reduce, a different mechanism related to contralateral effects must operate. Well, Dr Alf Breig provided a possible answer to this conundrum in 1960 with his observations of spinal cord and nerve root movement in cadavers. He showed that nerve root tension reduces when the spinal cord displaces caudad/downward in the canal (compare left and right sides of illustration). This produces a reduction in distance between exit point of the nerve root from the spinal cord and the intervertebral foramen, resulting in a reduction in tension in the nerve root.
As Shacklock (2005) proposed, it appears that it is this downward movement of the spinal cord that produces reduction in tension in the nerve roots. Additionally, the bilateral straight leg raise was shown to produce a reduction in symptoms with the MNT1 by Alison Bell in 1987. As far as we know, this was discussed at least verbally by Robert Elvey in the early 1980s, a significant observation that can now be applied clinically. The notion of reduction of tension with contralateral testing or use of the straight leg raise is now part of a progressional system proposed by Shacklock (2005, pp 156-158; Shacklock 2007).
In summary, the SLR may be used to reduce tension in the cervical nerve roots by moving the cord downward in the canal. Clinical application of this technique is potentially wide. It means that:
To learn how to perform these techniques safely, see course schedule.
Rubenach (1985) found that 62% of asymptomatic subjects reported a reduction in the symptom response to the median neurodynamic test 1 (MNT1) with performance of a contralateral MNT1. If we consider that tension in the nervous system is key the mechanism of symptoms with the MNT1, adding more tension to the nervous system with a contralateral neurodynamic movement should theoretically increase symptoms with the contralateral test. But, since the symptoms often reduce, a different mechanism related to contralateral effects must operate. Well, Dr Alf Breig provided a possible answer to this conundrum in 1960 with his observations of spinal cord and nerve root movement in cadavers. He showed that nerve root tension reduces when the spinal cord displaces caudad/downward in the canal (compare left and right sides of illustration). This produces a reduction in distance between exit point of the nerve root from the spinal cord and the intervertebral foramen, resulting in a reduction in tension in the nerve root.
As Shacklock (2005) proposed, it appears that it is this downward movement of the spinal cord that produces reduction in tension in the nerve roots. Additionally, the bilateral straight leg raise was shown to produce a reduction in symptoms with the MNT1 by Alison Bell in 1987. As far as we know, this was discussed at least verbally by Robert Elvey in the early 1980s, a significant observation that can now be applied clinically. The notion of reduction of tension with contralateral testing or use of the straight leg raise is now part of a progressional system proposed by Shacklock (2005, pp 156-158; Shacklock 2007).
In summary, the SLR may be used to reduce tension in the cervical nerve roots by moving the cord downward in the canal. Clinical application of this technique is potentially wide. It means that:
- in certain circumstances, lower limb movements can be used to ease pain and mobilise the nerve roots, including thoracic and cervical regions
- this produces a series of progressions which, for low back and sciatica are described in the last article on this subject
- lower limb movements can substitute contralateral upper limb neurodynamic testing, consistent with IN-OUT position and movement system provided in the last article and are described in more detail in (Shacklock 2005, Clinical Neurodynamics, updated in the NDS course manual, 2007).
- if, for instance, the contralateral MNT1 does not relieve a patient’s neck and or upper limb pain, the SLR can be applied instead.
To learn how to perform these techniques safely, see course schedule.
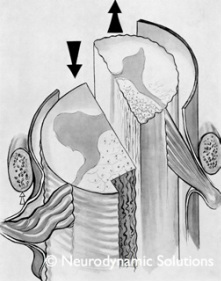
Left - Downward (caudal) movement of the spinal cord producing a reduction in tension in the nerve roots (from Breig 1960, Shacklock 2007a, © NDS 2007). Straight leg raise treatment for 'neural tension dysfunction' in the cervical nerve root (for classification, see Shacklock 2005, pp 60-61, English version).
It is hypothesized that the SLR pulls the cord downward in the canal which produces a reduction in tension in the cervical nerve root.
There is a progressional system for including both contralateral neural techniques and lower limb movements to reduce tension in the cervical nerve root (for progressions and definition of the 'neural tension dysfunction' see Shacklock 2005; 2007b). In the case illustrated, the nerve roots are placed under a certain degree of tension whilst the leg movements are used to decrease the nerve root tension from this position. However a lower and less provocative progression would be to NOT perform the upper limb neurodynamic movements and instead perform the mobilisation using the legs in isolation.
REFERENCES
Bell A 1987 The upper limb tension test and straight leg raising. In: Proceedings of the 5th Biennial Conference of the Manipulative Therapists' Association of Australia, Melbourne: 106-114
Breig 1960 Biomechanics of the central nervous system. Almqvist and Wiksell, Stockholm
Rubenach H 1985 The upper limb tension test — the effect of the position and movement of the contralateral arm. In: Proceedings of the 4th biennial conference of the Manipulative Therapists' Association of Australia: 274-283
Shacklock M 2005 Clinical Neurodynamics: a new system of musculoskeletal treatment. Elsevier, Oxford
Shacklock 2007a Shacklock M (Ed.) Biomechanics of the Nervous System: Breig revisited, NDS Neurodynamic Solutions, Adelaide
Shacklock M 2007b Clinical Neurodynamics Course Manual. Neurodynamic Solutions NDS, Adelaide
It is hypothesized that the SLR pulls the cord downward in the canal which produces a reduction in tension in the cervical nerve root.
There is a progressional system for including both contralateral neural techniques and lower limb movements to reduce tension in the cervical nerve root (for progressions and definition of the 'neural tension dysfunction' see Shacklock 2005; 2007b). In the case illustrated, the nerve roots are placed under a certain degree of tension whilst the leg movements are used to decrease the nerve root tension from this position. However a lower and less provocative progression would be to NOT perform the upper limb neurodynamic movements and instead perform the mobilisation using the legs in isolation.
REFERENCES
Bell A 1987 The upper limb tension test and straight leg raising. In: Proceedings of the 5th Biennial Conference of the Manipulative Therapists' Association of Australia, Melbourne: 106-114
Breig 1960 Biomechanics of the central nervous system. Almqvist and Wiksell, Stockholm
Rubenach H 1985 The upper limb tension test — the effect of the position and movement of the contralateral arm. In: Proceedings of the 4th biennial conference of the Manipulative Therapists' Association of Australia: 274-283
Shacklock M 2005 Clinical Neurodynamics: a new system of musculoskeletal treatment. Elsevier, Oxford
Shacklock 2007a Shacklock M (Ed.) Biomechanics of the Nervous System: Breig revisited, NDS Neurodynamic Solutions, Adelaide
Shacklock M 2007b Clinical Neurodynamics Course Manual. Neurodynamic Solutions NDS, Adelaide