The DANGER of IGNORING NOCICEPTION: Read THIS
This patient is a CHRONIC PAIN SUFFERER
Eight things we are told about pain:
So, this is WHAT I DID:
So I BROKE THE RULES and IT WORKED because, in this case, ALL of them were WRONG.
If I had ignored the patient's pain, the tibialis posterior tendon would have broken, requiring surgical repair and hindfoot stabilisation.
In summary:
- PAYING ATTENTION to the pain WORKED
- pain INDICATED that something was WRONG in the TISSUES
- PALPATION WORKED
- RADIOLOGY WORKED
- less movement, PROTECTING THE TISSUES from further damage WORKED
- SURGERY WORKED.
Now rehab is BACK ON TRACK.
This is an extreme case but IS IT EMBLEMATIC of many more complex and subtle MSK conditions about which we know very little? This relates to radiculopathy and disc protrusion. We are now advised that even radiculopathies often don't hurt.
TAKE HOME POINTS:
- generalisations about pain are often wrong
- it's about careful open-minded EVALUATION of EACH PATIENT - without bias.
- patients are full of surprises, so be prepared.
Eight things we are told about pain:
- nociception and pain are not the same thing
- pain is not an indication that something is wrong in the tissues
- paying attention to your pain will make it worse so focus on something else
- palpation is inaccurate so there's no need to do it
- pain and pathomechanics don't correlate, so don't worry about pathomechanics
- no need to do radiology either because pain and pathology don't match and it will create fear and dependence on tissue-based treatment
- don't fear movement, continue your rehab and be active. This will desensitise which is good.
- surgery is mainly placebo and, since pathology and pain don't match, don't even go there.
So, this is WHAT I DID:
- PAID ATTENTION to the pain
- BECOME CONCERNED that something was wrong in the tissues
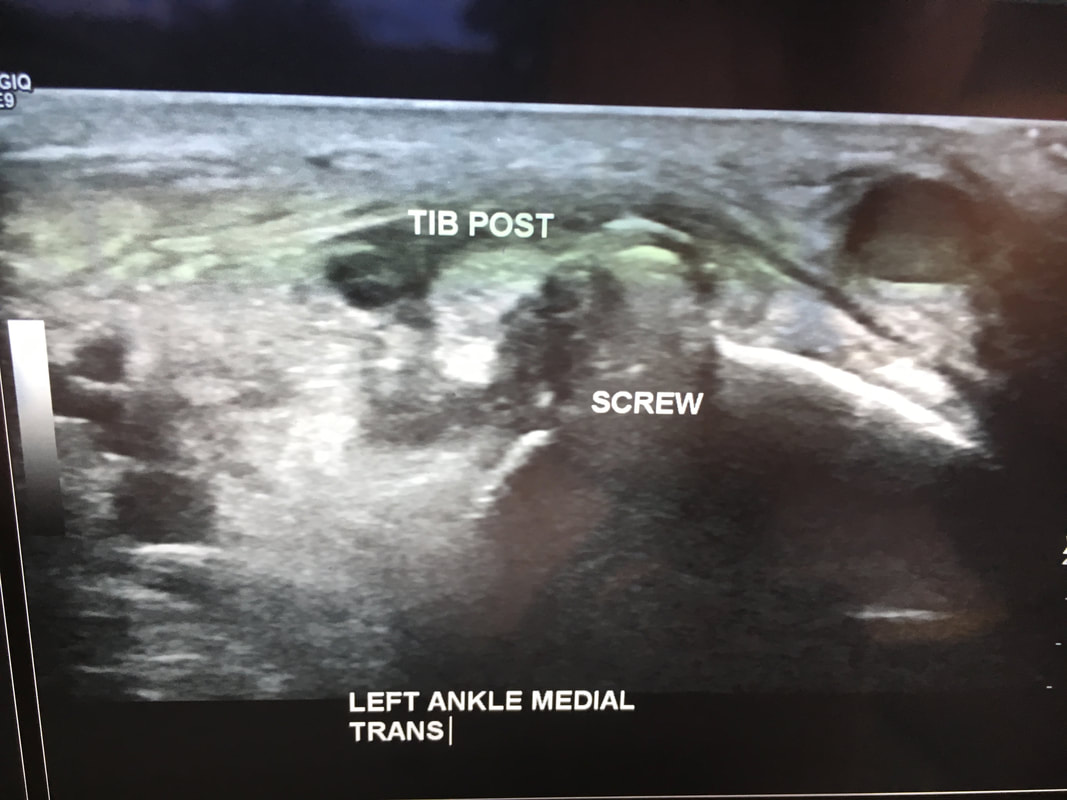
- PALPATED the area that hurt and found swelling in the tibialis posterior tendon and, right next to it over the tibia, a small, hard lump. Thought "Could this be a tendinopathy caused by pressure from the lump?"
- GOT RADIOLOGY and found the pathology and pathomechanics
- a SCREW from ankle surgery was IMPINGING on the tibialis posterior TENDON
- got CONCERNED that more WALKING would DAMAGE the tendon, so gave the patient a MOON BOOT to AVOID MOVEMENT and PROTECT the tendon
- SURGERY done to remove the screw. It had partially cut through the tendon.
So I BROKE THE RULES and IT WORKED because, in this case, ALL of them were WRONG.
If I had ignored the patient's pain, the tibialis posterior tendon would have broken, requiring surgical repair and hindfoot stabilisation.
In summary:
- PAYING ATTENTION to the pain WORKED
- pain INDICATED that something was WRONG in the TISSUES
- PALPATION WORKED
- RADIOLOGY WORKED
- less movement, PROTECTING THE TISSUES from further damage WORKED
- SURGERY WORKED.
Now rehab is BACK ON TRACK.
This is an extreme case but IS IT EMBLEMATIC of many more complex and subtle MSK conditions about which we know very little? This relates to radiculopathy and disc protrusion. We are now advised that even radiculopathies often don't hurt.
TAKE HOME POINTS:
- generalisations about pain are often wrong
- it's about careful open-minded EVALUATION of EACH PATIENT - without bias.
- patients are full of surprises, so be prepared.